

Abstract

Background: IVO (Agios Pharmaceuticals, Inc.) and ENA (Celgene) are small molecules approved by the FDA for treatment of adults with R/R AML with an IDH1 or IDH2 mutation, respectively. Gain-of-function mutations in IDH1 and IDH2 alter normal DNA methylation and impair differentiation (Im et al, Leukemia 2014). IVO and ENA inhibit IDH1 and IDH2 gain-of-function mutant enzymes, respectively, with the intent of restoring differentiation. IVO and ENA carry boxed warnings for differentiation syndrome (DS), a clinical syndrome that can be fatal if not treated. Montesinos et al (Blood 2009) proposed diagnostic criteria for DS based on at least 2 of the following signs and symptoms: 1) dyspnea, 2) unexplained fever, 3) weight gain, 4) unexplained hypotension, 5) acute kidney injury, and 6) pulmonary infiltrates or pleuropericardial effusion. Patients with 2 or 3 criteria were classified as having moderate and patients with at least 4 criteria were classified as having severe DS. DS was excluded in cases with an alternative explanation (e.g. septic shock). The incidence of DS in patients treated with IVO (DiNardo et al. NEJM 2018) and ENA (Fathi et al. JAMA Oncol 2018) has been reported based on investigator and review committee determination. FDA sought to perform a systematic analysis of DS cases in patients treated with IVO or ENA based on adverse event (AE) preferred terms (PTs) and laboratory test results grouped per the Montesinos criteria. We hypothesized that using an algorithmic approach would uncover a higher incidence of DS than reported initially.
Methods: We searched for cases of DS in Study AG120-C-001 for IVO and Study AG221-C-001 for ENA using PTs and laboratory data within the first 90 days of treatment, grouped per the Montesinos criteria. Patients were included in the analysis if they had been treated for R/R AML using the approved dose of IVO (n=179) or ENA (n=214). We reviewed case narratives and laboratory data for algorithmically-identified cases of DS to adjudicate whether cases were DS or unlikely DS, due to an alternative explanation (e.g., infection, disease progression). An additional query for the DS cases was performed for concomitant leukocytosis, defined using PTs Leukocytosis, Hyperleukocytosis, or White blood cell count increased, or laboratory results showing leukocyte count > 10Gi/L within 7 days of clinical signs/symptoms.
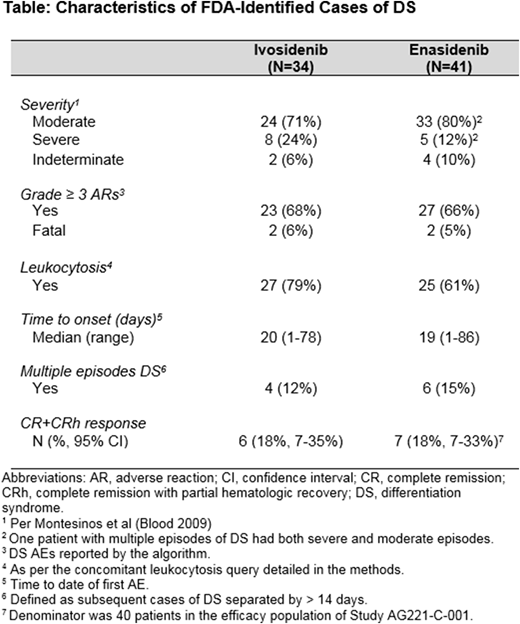
Results: The algorithm identified 72/179 (40%) cases of potential DS for IVO and 86/214 (40%) for ENA. FDA reviewer adjudication revealed that roughly half of the cases identified by the algorithm were DS for IVO (34/179, 19%) and ENA (41/214, 19%). This contrasts with the DS incidence of 11% (19/179) for IVO (DiNardo et al. NEJM 2018) and 12% (26/214) for ENA (Fathi et al. JAMA Oncol 2018) reported by investigators and review committee determination, respectively. Characteristics of FDA-identified DS cases in patients treated with IVO and ENA and FDA-adjudicated complete remission (CR) + CR with partial hematologic recovery (CRh) responses to the respective drugs in patients with DS are presented in the Table. For both IVO and ENA, CR+CRh rate in patients with DS was numerically lower than that for patients without DS (IVO: 18% [95% CI 7-35%] vs. 36% [95% CI 28-45%]; ENA: 18% [95% CI 7-33%] vs. 25% [95% CI 18-32%]). Age, demographics, and cytogenetic risk of patients with FDA-identified DS were similar to those of patients without DS.
Conclusions: An algorithmic analysis of AEs and laboratory tests using the Montesinos criteria led to recognition of additional cases of DS not identified by investigators for patients treated with IDH inhibitors IVO and ENA. DS occurred in roughly one in five patients treated with both drugs and grade 3 or higher adverse reactions were present in over half of cases. Leukocytosis was not always present. Patients with DS had numerically lower response rates, but firm conclusions regarding the impact on response cannot be inferred based on this post-hoc subgroup analysis. Increased recognition of signs and symptoms of DS through the framework of the Montesinos criteria may lead to earlier diagnosis and treatment, which may decrease severe complications and mortality. Furthermore, integration of the algorithmic approach into clinical trials of differentiating therapies may help to prospectively monitor the incidence and severity of DS.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal